Dr Rangan Chatterjee chats with Dr Gabor Maté about his radical findings based on decades of work with patients. We’re currently living in a culture that doesn’t meet our human needs. Maté and Chatterjee delve into how our emotional stress can translate into physical chronic illnesses, and how loneliness and a lack of meaningful connection are on the rise, as are the rates of autoimmune disease and addiction.
Related Post
Polyvagal Theory and Trauma – Dr. Stephen PorgesPolyvagal Theory and Trauma – Dr. Stephen Porges
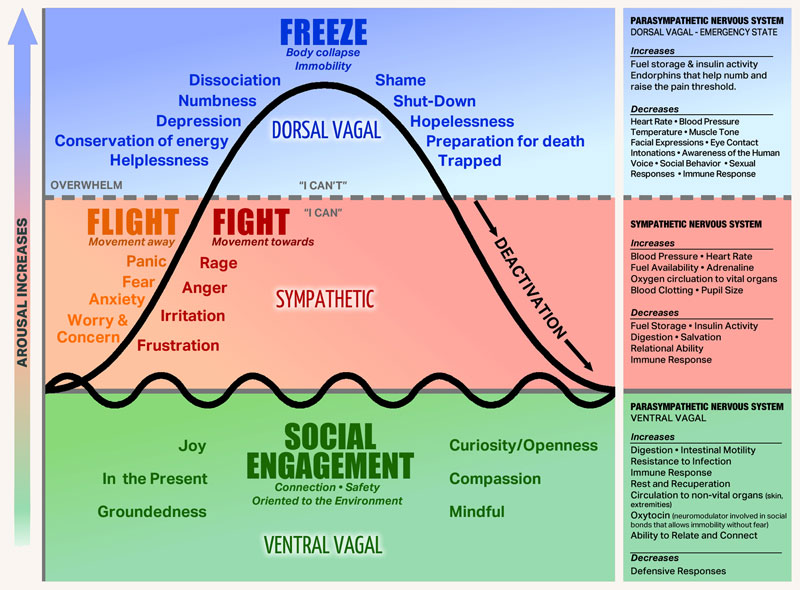
Stephen Porges, psychiatry professor and researcher, on the polyvagal theory he developed to understand our reactions to trauma:
[Paraphrased] Polyvagal theory articulates three branches of the autonomic nervous system (ANS) that evolved from primitive vertebrates to mammals. First, there is a system known as ‘freeze’, which involves death feigning or immobilisation. Second, the ANS has a ‘fight or flight’ system, which is a mobilisation system. And third, with mammals, there is what Porges calls, a social engagement system (SES), which can detect features of safety, and actually communicate them to another. The SES may also be referred to by some as ‘rest and digest’, which Porges theory suggests is a function of the Vagus Nerve – the tenth cranial nerve, a very long and wandering nerve that begins at the medulla oblongata. When an individual experiences feelings of safety (within an SES state), the autonomic nervous system can support health restoration. In terms of dealing with a life threat, an ordinary person will most likely go into a feigning death, dissociative state of ‘freeze’.
Polyvagal theory in psychotherapy offers emotional co-regulation as an interactive process between therapist and client which engages the social engagement system of both therapist and client. Social engagement provides experiences of safety, trust, mutuality and reciprocity in which we are open to receiving another person, just as they are.
The following extract has been retrived from https://www.theguardian.com/society/2019/jun/02/stephen-porges-interview-survivors-are-blamed-polyvagal-theory-fight-flight-psychiatry-ace
Polyvagal theory has made inroads into medical and psycho-therapeutic treatment, but how should it inform how people treat each other?
“When we become a polyvagal-informed society, we’re functionally capable of listening to and witnessing other people’s experiences, we don’t evaluate them. Listening is part of co-regulation: we become connected to others and this is what I call our biological imperative. So when you become polyvagal-informed you have a better understanding of your evolutionary heritage as a mammal. We become aware of how our physiological state is manifested, in people’s voices and in their facial expression, posture and basic muscle tone. If there’s exuberance coming from the upper part of a person’s face, and their voice has intonation modulation or what’s called prosody, we become attracted to the person. We like to talk to them – it’s part of our co-regulation.
So when we become polyvagal-informed, we start understanding not only the other person’s response but also our responsibility to smile and have inflection in our voice, to help the person we’re talking to help their body feel safe.”
Clink on the link below to hear Dr. Bessel van der Kolk, one of the world’s leading experts on developmental trauma, explain how our long-term health and happiness can be compromised by prior exposure to violence, emotional abuse, and other forms of traumatic stress.
Australian Institute of Professional Counsellors. (2021). Finding Meaning: Masculinity in Crisis (Issue 358 // Institute Inbrief). Retrieved from https://mailchi.mp/aipc/institute-inbrief-179116?e=5e8ce9018dAustralian Institute of Professional Counsellors. (2021). Finding Meaning: Masculinity in Crisis (Issue 358 // Institute Inbrief). Retrieved from https://mailchi.mp/aipc/institute-inbrief-179116?e=5e8ce9018d
Finding Meaning: Masculinity in Crisis
Many young men seek counselling because they feel lost (Seidler, et al., 2016). This happens especially in today’s world, where the boundaries of how a man is supposed to behave are shifting rapidly. It’s a difficult time for young men to find their place in life as they struggle to adapt themselves to changing social attitudes and norms; there’s plenty of content in the media illuminating harmful male behaviours, but there isn’t a legitimate mainstream discussion of how masculinity ought to be propagated. As a result, many young men are growing into adulthood without a map – they lack a male voice of compassion and authority to guide them on how to integrate masculinity into their lives.
In our writer’s experience, men who have been referred for counselling often have a very strong underlying sense of purpose and a desire to be good people; their anxiety, depression, and harmful behaviours are often symptoms of feeling unable to actualise their potential. It’s a counsellor’s job to help men articulate this sense of purpose in constructive and positive ways, and offer guidance on enacting their perceived purpose effectively.
A study from the University of Connecticut has identified three major factors that determine whether men believe their lives are meaningful (George & Park, 2016):
- They feel that their lives make sense, and have continuity
- They are directed and motivated by meaningful goals
- They believe their existence matters to others
Researchers discovered that sources of meaning tend to fall into two main categories: meaningful relationships and a meaningful profession (George & Park, 2016).
There is no doubt that this generation of males is developing a unique relationship with masculinity, and it’s not necessarily for the betterment of their relationships or professions (Black & Westwood, 2012); men’s desire for professional success can be interpreted as a validation of the patriarchal system, while their pursuit of romantic relationships can be perceived as misogynistic (LeanIn, 2019). While some men are certainly exploiting systems which privilege them, often times the prevalence of this attitude discourages “good” men from progressing and developing themselves (Hoff, 2016). This article is not making a stance on any social/political issues: it is merely articulating some causes and concepts that can assist counsellors in understanding this very nuanced issue, so they can help men find meaning in the modern world.
What even is masculinity?
Masculinity and femininity denote sets of attributes that most people can intuitively identify – for example, it doesn’t take a discerning anthropologist to tell the girls section of the toy store apart from the boys section. But regardless of the value of this distinction, what exactly is the nature of it? Defining masculinity and femininity is a little more nuanced than simply referring to their apparent differences; not all people have the same understanding of what masculinity and femininity are, and how they manifest themselves. For example, conceptualisations of masculinity and femininity vary vastly across cultures and historical periods (Reeser, 2010); as such, there can be confusion about what these terms mean, and how we can embody them effectively.
Across time, however, typically agreed-upon standards for masculine conduct involve strength, courage, and leadership (Kimmel, 1994); these traits reflect a desire for meaning – you only inhabit strength and courage when a compelling reason to do so arises. Young men today, knowingly or not, are crying out for responsibilities that offer this type of meaning in their lives (Frankl, 2006). They want to know what it means to be who they are in the world right now – what can they do, and how can they best live? It’s time that we help them find the answers to these questions.
Currently, there is a lot of heated discussion about whether masculinity – or any kind of gender categorisation – is a genuine natural occurrence, or a mere social construction that we can/should dispose of; the question of whether masculinity is inherent in biology or if it arises through socialisation has been debated for hundreds of years (Martin & Finn, 2010). This is a question that does not have a black-and-white answer; studies on prenatal androgen exposure – among other developmental events – have shown biological links to expressions of masculine or feminine traits (Martin & Finn, 2010), however, it can be argued that these differences are exaggerated and articulated further by social influences (Wharton, 2012).
Whichever perspective you align with, an often unacknowledged aspect of these conversations is that while some forms of masculinity are harmful, some are also powerful forces for good. It’s possible (and advised) for men to have a productive and integrated expression of their masculinity (Jung, 2009) – one that allows them to use their strengths to achieve fulfilment. Unfortunately, the current culture is lacking in content which identifies what these strengths are, and thus fails to encourage men to embody them; as detailed above, many young men feel lost because of this.
It should also be stated that masculine traits are not exclusive to men; masculinity and femininity are not synonymous concepts to gender or sexual identity (Butler, 2006). That being said, this article is specifically addressing the mental health of men with masculine attributes.
Why is masculinity in crisis?
There are a variety of reasons why young men feel uncertain about how to navigate the contemporary world. These include, but are not limited to, the following 3 observations:
1) The increasing separation between traditional male roles and the reality of modern life
The roles of men in the traditional household and workplace are changing. Men are becoming more inclined to be actively involved in child-rearing and housework. However, there is still often an expectation for them to maintain the traditional breadwinner role (Martin & Gnoth, 2009). Men are finding themselves stuck in limbo between the past and the future. Discerning one’s purpose thus becomes difficult, leading to feelings of emptiness (Rogers, 2010); men without a defined mission will generally find themselves feeling a tremendous sense of lack (Deida, 1997). In this day and age, young men are extremely worried about what they will do after college, and the answer is likely “Go overseas for a few years, then come back.” This reflects a lack of encouragement to make powerful decisions towards meaningful futures.
2) A lack of positive masculine role models in society
For many children, fathers are either absent or not present enough, and this has lasting impacts on the way males view themselves and their sense of meaning/purpose in the world (Single Mother Guide, 2012). Men who grow up without an emotionally involved father has been correlated with long term effects including increased likelihood of dropping out of high school or college, and increased likelihood of substance abuse (McLanahan, Tach, & Schneider, 2014). These problems are exacerbated by the fact that many young men are searching for their place in the world and attempting to figure out what it means to be a man in today’s society – there is not always an adult male figure for them to look up to.
The men who are often placed in the media limelight are there by way of some transgression or moral failing. While the modern world is rightly campaigning for positive representations of identities in media, it seems as though this effort circumvents men (Tarrant, et al., 2015). It is understood that men have historically tended to see themselves in positions of power and dominance, but this is not a reason to avoid exposing men to genuinely positive role-models in our current time. It is to the detriment of the mental health of many young men that we do not see more positive representations of masculinity (Tarrant, et al., 2015); ones that represent the compassionate and purposeful core of the masculine ideal.
3) Social media content either teaches men harmful ways of interacting with others, or degrades the concept of masculinity in general
The following two types of social media content are tough for today’s men to navigate. Firstly, there is a large online community of content creators calling for men to be ruthlessly successful; young men are bombarded with images of ‘alpha-males’ and are expected to adopt this image into their own definitions of masculinity. This makes it more difficult for boys to embrace their sensitive sides, leading to a lack of emotional literacy (Stratford, 2020). Content creators rarely offer antidotes to this effect, and are failing to provide helpful insights into the psychological reality of becoming a good man with a meaningful life. These online figures often try to convey an image that their life is perfect, when in fact this is often far from the truth; men are being encouraged to strive for false images of fulfilment (Stratford, 2020). This is a major concern for both men and women.
Secondly, while some men are being plagued by the alpha-male image, others are being exposed to content that degrades masculinity in general. The conduct of certain men has been the object of fair scrutiny over recent years, and there are arguments to be made for how this conduct has been an expression of masculinity. There is, however, no grounds for suggesting that masculinity in general is problematic. This view has created a culture in which masculinity is demonised; while this might be a perceived course-of-action for eradicating its more toxic forms, the more immediate effect is that good men are feeling alienated and ineffectual (Rogers, 2010). Rather than encouraging men to be better, we are constantly reminding them that they are harmful; a result of this is a generation of men who are unmotivated and aimless (Salter, 2019). A study has found that male respondents who have experienced gender-based cyberbullying feel compromised in how they feel they are permitted to exist in society (Chen, et al., 2015). Men are seen as less attractive and less desirable to women when they post images of themselves on their Instagram account, as it is seen as the promotion of male dominance rather than a harmless expression of an individual (Fox & Rooney, 2015). This phenomenon leads to a significant decrease in men’s self-esteem, which results in paralysis and stagnation in their professions and relationships.
So, how can counsellors help men find purpose and meaning?
As counsellors, we can offer strategies to help men identify and organise the meaningful facets of their lives. Viktor Frankl, the author of Man’s Search for Meaning, created logotherapy, which is based on the presumption that a man’s main motivation is to find meaning in life, as opposed to the pursuit of pleasure or power (Marshall & Marshall, 2012). Some techniques he used were dereflection (focusing on high-level goals instead of on themselves) and Socratic dialogue (open-ended questions to uncover dormant aspirations). If, for example, a client is passionate about saving the environment, this type of therapy can assist them in finding a practical way to focus their time and efforts on realising their potential in doing so.
Meaning therapy (Wong, 2010) incorporates aspects of cognitive-behavioural therapy and positive psychology, and helps people take on more meaningful responsibilities in their lives while encouraging them to pursue goals that serve others. It advocates psycho-educational approaches that equip men with the mental toolkit necessary to create a vision of an idealised future for them to begin moving towards.
Similarly, self-authoring is a process by which people organise their lives into a narrative structure, making their past, present, and desired futures more easily understandable (Peterson, 2005). By creating a map of one’s life, it can become far simpler to identify who you are, what you value, and what you need to do to be of most service to yourself and your community. As with most approaches that attend to creating meaning, it is based on reflection and awareness.
A culture of masculine content creation must be encouraged to counter the fear of being construed as ‘too emotional’, or ‘not manly enough’. It’s time we begin working together to help young men find meaning, and develop a culture which is focused on stopping the cycles of toxic masculinity, whilst encouraging healthy expressions of masculinity in its stead.
In summary…
Young men today are having a difficult time finding their place in the world. The current cultural climate surrounding masculinity – as well as the absence of positive role-models for younger generations – is leading to a decrease in the quality of mental health. Men must be taught how to integrate their masculine dispositions into their lives; how to lead, how to care, and how to love with purpose and commitment. There is an urgent need for discussion to take place around what masculinity means, and how we can encourage healthy expressions of it; it is my hope that this article has encouraged us all to begin engaging with this conversation.
Recommended Links: Men In Mind Program (by Movember), Men and Emotions: From Repression to Expression (Article), Men, Emotions and Alexithymia (Article)
References:
- Butler, Judith (2006) [1990]. Gender trouble: feminism and the subversion of identity. New York London: Routledge.
- Cunningham, C. E., Chen, Y., Vaillancourt, T., Rimas, H., Deal, K., Cunningham, L. J., & Ratcliffe, J. (2014). Modeling the anti‐cyberbullying preferences of university students: Adaptive choice‐based conjoint analysis. Retrieved from webpage.
- Deida, D. (1997). The Way of the Superior Man. S.I.: Sounds True.
- Fox, J., Rooney, M. (2015) The Dark Triad and trait self-objectification as predictors of men’s use and self-presentation behaviors on social networking sites. Personality and Individual Differences
- Frankl, V. E., Kushner, H. S., & Winslade, W. J. (2006). Man’s search for meaning. Boston, MA: Beacon Press.
- Hoff, C. (2016). Five Ways Patriarchy Affects Men and their Relationships. Retrieved from webpage.
- Jung, C. G., Shamdasani, S., & Hoerni, U. (2009). The red book = Liber novus: A readers edition. New York: W.W. Norton &.
- Kimmel, Michael S. (1994). “Masculinity as Homophobia: Fear, Shame, and Silence in the Construction of Gender Identity”. Theorizing Masculinities. Thousand Oaks: SAGE Publications, Inc. pp. 119–141.
- LeanIn.Org and SurveyMonkey survey (2019)
- Maria Marshall; Edward Marshall (2012). Logotherapy Revisited: Review of the Tenets of Viktor E. Frankl’s Logotherapy. Ottawa: Ottawa Institute of Logotherapy.
- Martin, Brett A.S.; Gnoth, Juergen (2009). “Is the Marlboro man the only alternative? The role of gender identity and self-construal salience in evaluations of male models”. Marketing Letters. 20 (4): 353–367.
- Martin, Hale; Finn, Stephen E. (2010). Masculinity and Femininity in the MMPI-2 and MMPI-A. University of Minnesota Press. pp. 5–13.
- McLanahan, S., Tach, L., & Schneider, D. (2013). The Causal Effects of Father Absence. Retrieved from webpage.
- Peterson, J. (2005). Self Authoring. Retrieved from https://www.selfauthoring.com/
- Reeser, Todd W. (2010). Masculinities in theory: an introduction. Malden, Massachusetts: Wiley-Blackwell.
- Rogers, Thomas (November 14, 2010). “The dramatic decline of the modern man”. Salon.
- Salter, Michael (2019). “The Problem With a Fight Against Toxic Masculinity”. The Atlantic.
- “Single Mother Statistics”. Single Mother Guide. (2012)
- Seidler Z. E., Dawes A.J., Rice S. M., Oliffe J. L., Dhillon H. M. (2016). The role of masculinity in men’s help-seeking for depression: A systematic review. Retrieved from webpage.
- Stratford, H. (2020). ‘Be a man’ – toxic masculinity, social media and violence: Innovation Unit: Creating impact – reducing inequalities – transforming systems. Retrieved from webpage.
- Tarrant, A., Terry, G., Ward, M., Are Male Role Models Really the Solution? Interrogating the ‘War on Boys’ Through the Lens of the ‘Male Role Model’ Discourse. (2015). Retrieved from webpage.
- Westwood, M. J., & Black, T. G. (2012). Introduction to the Special Issue of the Canadian Journal of Counselling and Psychotherapy. Retrieved from webpage.
- Wharton, Amy S. (2012). The Sociology of Gender, second edition. Hoboken, NJ: Wiley-Blackwell.
- Wong, P. T. (2009). Meaning Therapy: An Integrative and Positive Existential Psychotherapy. Retrieved from webpage.